
Nancy Homewood from XLVets Equine explains an ongoing case that she’s been investigating recently
Last week, I was called to see a gelding who’d been showing intermittent signs of mild colic for a few days.
He’d been swishing his tail, acting restless and circling with his ears back and looking unhappy. When I first saw him, one of the first things that stood out to me was the discolouration on his hindlimbs.
He had a yellow-brown staining running down his grey coat on the inside and front of his legs. I took a full history and began my examination.
His vital signs were normal, but there were a few subtle abnormalities that began ringing alarm bells. He was constantly twitching his ears backwards and forwards and had a slightly low head carriage.
His coat was a bit dull and he was slightly underweight for his big frame. When I examined his underside and sheath, I noticed he was dribbling a small amount for urine from the tip of his urethra.
The staining down his hind limbs was in fact urine, and it contained a lot of chalky sediment. When I spoke to the owner about the horse, he told me he had always been a ‘dirty’ horse and would often walk away from a urinating stance, still dribbling urine occasionally.
My suspicions were that we may be dealing with something that the horse had been compensating for over some time and it had hit a critical point where he was starting to show more advanced clinical signs.
Further investigation
I took a blood sample and administered some anti-inflammatory medication and asked the owner to collect a urine sample from the horse.
The blood sample was taken to check for normal kidney function and any signs of systemic disease. It didn’t show any abnormalities, but the urine sample had large amounts of calcium carbonate.
Excessive calcium carbonate is excreted by the horse in the urine and varying amounts can be found in ‘normal’ horse’s urine, giving it that cloudy appearance towards the end of urination. However, in this horse’s case, the urine was saturated with calcium carbonate.
Calcium carbonate accumulates in the bladder for a number of reasons, the most common being lack of bladder tone and function. This causes a failure in the complete ‘emptying’ of the bladder – leaving calcium carbonate sediment sitting at the bottom of the bladder.
Control of bladder function in horses is complex and problems can be caused by a number of underlying factors, including nerve damage inflammation. The gelding showed no lameness or neurological deficits and due the chronicity of his disease, it’s unlikely we’ll ever know the exact underlying cause of the loss of bladder tone.
He was admitted to the equine clinic for further investigations. We examined him in stocks to reduce the risk of injury and an internal ultrasound examination revealed a bladder largely full of sediment.
The gelding was sedated and we gave him muscle relaxants and pain relief, and catheterised his bladder. It was apparent under sedation that his penis had areas of ulceration where his urine had scalded the skin.
When we first catheterised his bladder, we collected five litres of thick, chalky urine.
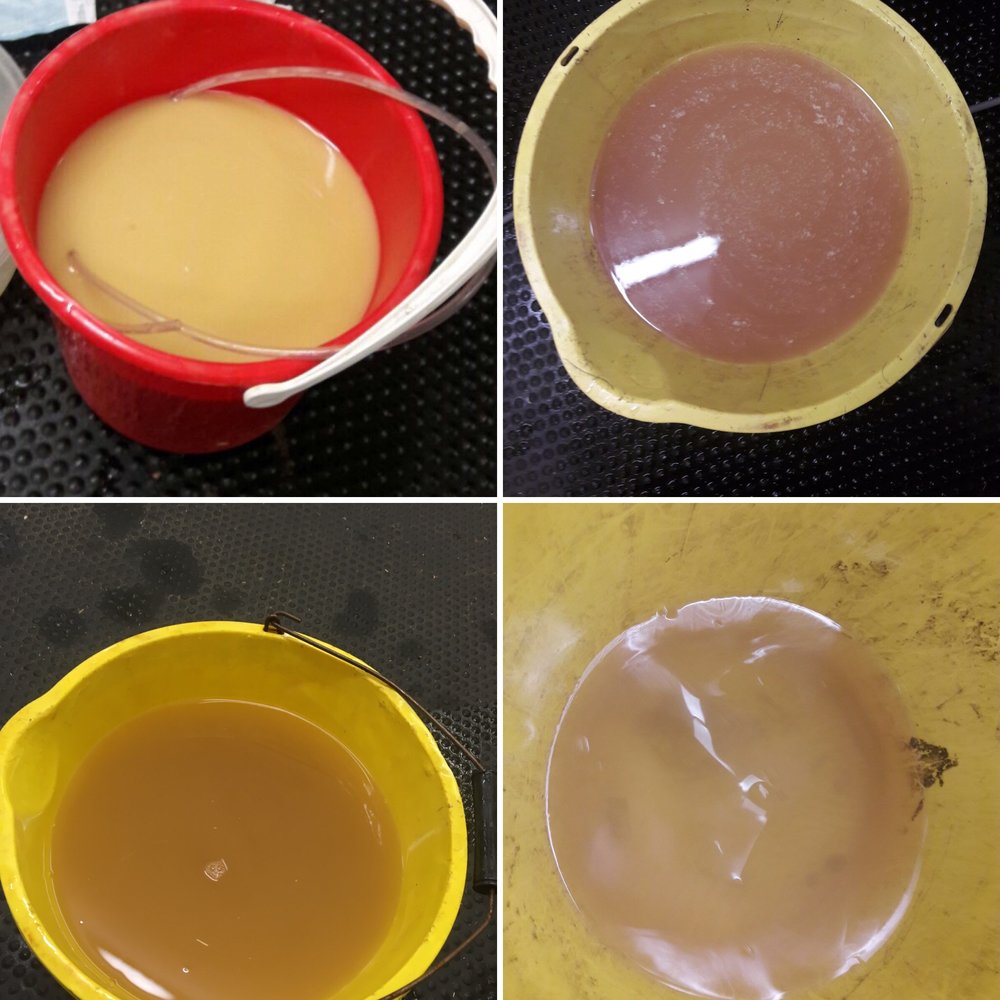
I then lavaged the bladder to attempt to dilute and dislodge the chalky material. Once we’d lavaged the urine from the bladder, an endoscope was passed up his urethra to visualise the urethra and the inside of the bladder.
Looking inside
The lining of the bladder was inflamed with areas of haemorrhage and ulceration. Despite lavaging, a large plaque of chalky sediment remained at the bottom of the bladder.
Over the next week, the gelding had his bladder lavaged daily to attempt to dislodge the calcium carbonate and reduce the inflammation and irritation within his bladder.
He was given anti-inflammatories and antibiotics, as well as a Vitamin C supplementation to help acidify the urine.
Over the course of the week, he improved in demeanour and gained 20kg in weight. There was less urine scalding on his hindlimb and his urine became more ‘normal’ as the week progressed.
At times he urinated normally and at others he was seen to dribble urine seemingly unconciously when stood. In my experience, these cases need ongoing management and are unlikely to fully resolve.
Once the bladder tone is lost, it can be difficult to improve. The mainstay of treatment is to provide anti-inflammatories and pain relief as necessary, dietary modification to reduce calcium intake (cutting out alfalfa and concentrates that are high in calcium) and lavaging the bladder to help dilute and remove the calcium carbonate that accumulates there.
He’s due back in three weeks time to have a repeat bladder scope and lavage – I’ll keep you up to date with his progress!






